
Written by Hiroyuki Noguchi
English Version
HFNC may appear to be a form of oxygen therapy; however, its true essence lies in supporting respiration through flow.
In this article, the mechanism of HFNC is organized from the perspective of Flow Assist & Flow Resistance.
This article is the English version of a concept originally published in Japanese on March 12, 2026.
Characteristics of HFNC
= Flow Assist & Flow Resistance
Traditionally, the following five characteristics have been described for HFNC:
- Stable delivery of FiO₂ to the alveoli
- Washout of CO₂ from the upper airway dead space
- PEEP-like effect
- Comfort provided by heated humidification
- Reduction of the work of breathing
In addition, Flow Matching has been proposed as a method to maximize these characteristics.
Stable FiO₂ delivery, dead space washout, and the benefits of humidification can be explained by the flow rate and concentration of the inspired gas.
However, regarding the so-called “PEEP-like effect,” I questioned whether true PEEP is actually generated at the alveolar level.
Observations using EIT (Electrical Impedance Tomography) have demonstrated that HFNC increases FRC (Functional Residual Capacity).
However, this increase does not necessarily correspond to the pressure measured in the nasopharynx.
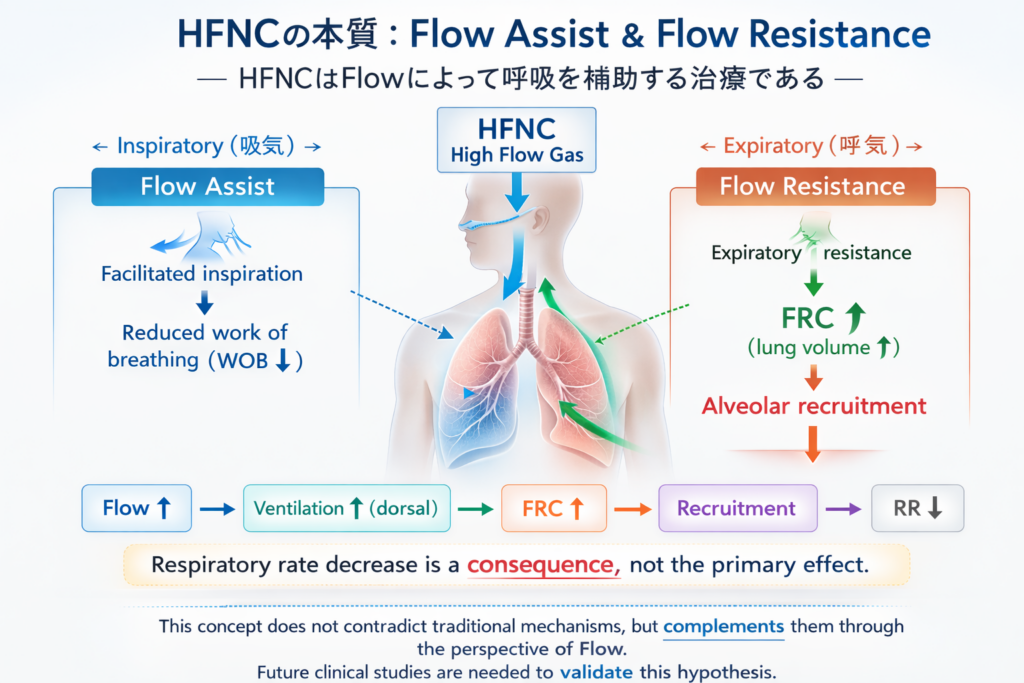
Flow Assist & Flow Resistance
This led to the concept of “Flow Assist & Flow Resistance.”
During inspiration, HFNC delivers a flow rate that exceeds the patient’s inspiratory demand.
This facilitates inspiration and functions as Flow Assist.
On the other hand, the high flow continues even after inspiration has ended.
As a result, resistance occurs against the expiratory flow.
This resistance to expiration can be interpreted as Flow Resistance.
Because of this expiratory resistance, gas tends to remain in the lungs at the end of expiration, which may lead to an increase in FRC.
As a consequence, alveolar recruitment may occur, improving ventilation-perfusion matching and ultimately resulting in a reduction in respiratory rate.
zechanism consisting of:
Flow Assist (inspiration)
Flow Resistance (expiration)
Background of the Concept
The motivation for developing this concept came from three sources:
- my personal experience using HFNC
- observations obtained from EIT (Electrical Impedance Tomography)
- feedback from patients
In my own experience, when HFNC was applied at 30–40 L/min, which roughly corresponds to the inspiratory flow during resting breathing, no significant change in breathing was observed.
However, when the flow was increased to 50–60 L/min, the breathing pattern changed from anterior chest dominant breathing to abdominal and dorsal dominant breathing, accompanied by a reduction in respiratory rate.
At the same time, changes in the EIT potential distribution were observed, suggesting that the ventilation distribution had changed.
In clinical practice, some patients report that “it becomes difficult to exhale” when the HFNC flow is increased.
In addition, there are cases in which increasing the flow does not produce the expected clinical improvement.
From these experiences and observations, I began to consider that the conventional explanations of HFNC might not fully explain these phenomena.
Therefore, I reorganized the mechanism of HFNC from the perspective of the respiratory cycle, leading to the concept of:
Flow Assist during inspiration
Flow Resistance during expiration
Accordingly, HFNC may be understood not simply as oxygen therapy, but as a therapy that supports breathing through flow.
Conclusion
The concept of Flow Assist & Flow Resistance presented in this article is a conceptual model that organizes the mechanism of HFNC from the perspective of flow.
This concept does not contradict the conventional understanding of HFNC mechanisms.
Rather, it may serve as a complementary framework that helps explain these mechanisms more clearly.
Further clinical research will be necessary to validate this concept and deepen our understanding of how HFNC works.